The Beginning
mNote started with
two MBA students and two PhD students who became interested in community
health workers. Our backgrounds are diverse: a mechanical engineer,
a former biomedical engineer, a one-time information architect, and
a marketeer. Two Americans, a Zimbawean, and a Peruvian. Two veterans
of the dSchool's Extreme
Affordability course;
two of us who had never taken a formal design course.
In the initial needsfinding reports, we were drawn to the tension
between how community health workers (CHW) saw themselves (as unpaid
but proud professionals nominated by their community) and how often
clinics or patients seemed unclear about the CHW's role in the larger
health ecosystem. This tension inspired our initial Point of View as
well as subsequent revisions and set us down the path that eventually
evolved into mNote.
Point of View
Okoth, a passionate but under-resourced
Community Health Worker needs a way to maximize his impact on his
patient’s overall well-being.
(The first part of our final presentation describes Okoth's story in more detail.)
Insights and Observations
from Needsfinding
We explored a variety
of solutions to address this point of view and empower CHWs to better
care for their patients: a system to streamline referral management
and post-visit follow up between clinics and CHWs, job aides to assist
CHWs visiting a sick patient in making the treat vs. refer decision,
and a patient notification system for when CHWs were not able to visit
as expected. As we discussed these ideas with community health workers,
NGO staff, and others knowledgeable about healthcare around Nairobi,
however, it became clear that each applied only to a tiny subset of
CHWs. Most community health workers work with multiple NGOs and thus
play multiple roles. One common denominator we identified, however,
is that they all need to gather and record information and that they
want to have control over how the collection happens. Currently information
is collected in a paper notebook, which the community health workers
use to track patients' progress, report activities to the NGOs with
whom they work, and share with other community health workers for professional
development.
Description of mNote
mNote is an online archive for community health worker notes. NGOs log onto the mNote website to create forms for their CHWs to fill out. mNote alerts each CHW to download the new form via SMS. When in an area with service, the CHW downloads the form via prepaid data on their midrange Nokia phone.
mNote allows the CHW
to rearrange the order of questions within the form to best match their
preferred workflow. MNote forms can contain prompted text entry fields
as well as multiple choice fields. The CHW uploads completed forms via
the same prepaid data connection approximately weekly, or whenever they
are in an area of data service.
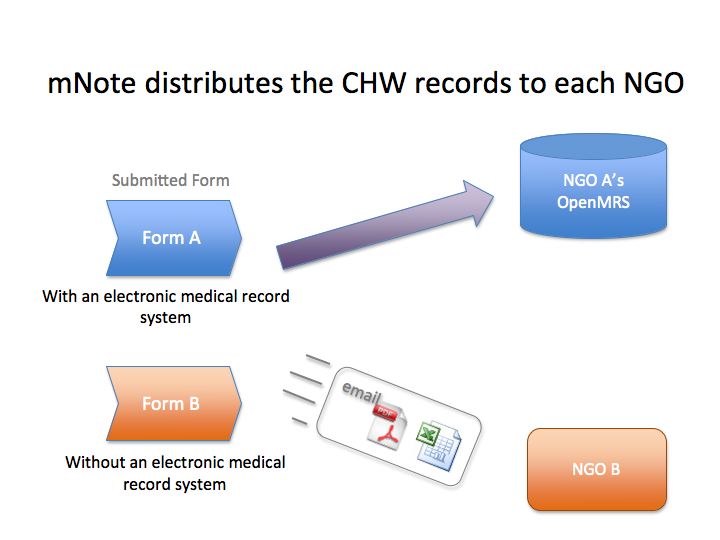
For NGOs with existing electonic medical record systems, such as the popular OpenMRS, uploaded forms are automatically synced with their server. NGOs without an electronic medical record system receive an email with the forms attached in spreadsheet or PDF format as a replacement for their former process of photocopying and interpreting the CHW's notebook. (Please see our final presentation for diagrams and more detail.)
Decisions and Insights
One of our key insights was that community health workers perform very different tasks, depending on the NGO that they are working for and which country they are located in. This has important implications:
Given these insights
and the diversity of perspectives we were hearing about CHWs' roles,
we chose to focus on a single CHW, Okoth, and make subsequent design
assumptions based on his experiences.
Assumptions We Made
(For more on the process
of developing materials, see our collection
of archived process materials).
Benefits of mNote
mNote empowers CHWs by preserving the flexibility and control they appreciate in their current paper notebooks, but adding digital knowledge management capabilities. The system allows CHWs to:
By creating a detailed
record of their activities, mNote also has the potential to enhance
the perception of community health workers as the professionals our
interviews and the initial needsfinding reports suggested they see themselves
to be.
While mNote, unlike other clinic-focused systems, is designed specifically for CHWs, it also provides significant benefits for NGOs who work with CHWs. By streamlining and integrating CHW data, mNote allows NGOs to:
Next Steps and Open Questions
One of our major concerns
in deciding that our user would be someone like Okoth is whether or
not he is a typical CHW, or whether our solution is out of the reach
of less literate CHWs. The approach that we have taken is to design
for a highly literate CHW who is comfortable with technology. mNote
could be made more suitable for CHWs who do not fit this description
by stripping or simplifying some of the functions so that they could
be used on a less sophisticated phone and require less training. Another
path we explored that would be a fruitful avenue for future prototyping
is a voice-based rather than text-based system, given the low literacy
and visual acuity reported among at least certain segments of the CHW
population, though not represented in the user for whom we were designing.
Our solution requires that a the mobile phone is linked to a data plan,
which implies both a higher end phone and most likely a significant
financial investment. However, there are options for transferring data
efficiently and cost effectively, as is demonstrated in a thesis by
Stanford student Tom Wiltzius - "__Mobile
Medic: Extending the Effective Reach of Mobile Data Infrastructure for
Data Collection Applications in Emerging Regions__"
(please contact Prof. Terry Winograd to obtain a copy).
An important next step
will be to identify an NGO who would benefit from mNote and seek a partnership
with them. An organisation like the Tabitha Clinic, managed by Carolina
for Kibera, is an excellent candidate, since they have already demonstrated
the willingness to adopt new technology. Initiating this partnership
would allow us to further understand the CHWs that our target clinic
employs, including their roles, educational level, workflow, etc.
By design, mNote's
user is the community health worker. However, CHWs are unlikely to have
sufficient funds to purchase the phone required or sufficient technical
training to set up and maintain the system. Therefore, a critical question
is who would be the ultimate "buyer" of this technology. NGOs
may resist investing in a system that gives most of the benefit to CHWs
without also deriving benefit for the NGO as well, so there would need
to be a clear value proposition from the point of view of the organization.
However, we believe that adoption of mNote by NGOs can be driven by
their funders or by organizations whose mandate is to improve the efficiency
of NGOs. For instance, a large funding organization such as the Gates
Foundation could conceivably require that a system like mNote be used
as a prerequisite for funding. Another possibility would be a job creation
or community development focused NGO, who might be interested in mNote's
potential to professionalize the work of CHWs by providing records of
what they do and thus answer the common argument against paying them,
which is that there is no accountability in their activities.